Authors: Andrew Schroeder, Lauren Bateman, John Crowley, Satchit Balsari, Nishant Kishore, Jennifer Chan
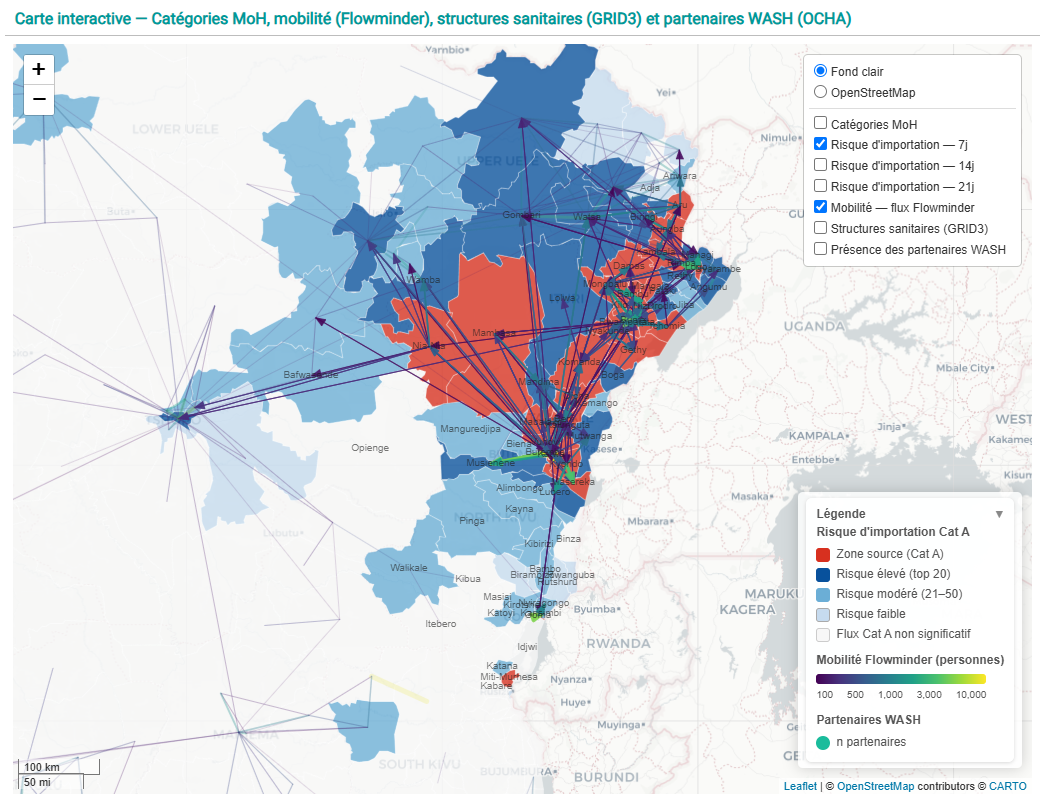
Map: Movement flows of people through Ituri and Kivu districts, shaping the potential risk landscape for spread of Bundibugyo Ebola Virus in DRC. Data from Flowminder, based on mobile devices from Vodacom. Dashboard produced by iMMAP for the WASH Cluster.
Source: https://immap.org/country-programs/global-wash-cluster-field-support-team-consortium-member
As of the week of June 15th, 2026 one of the largest outbreaks of the Ebola virus in history continues to grow with alarming speed. According to the latest INSP (Government of DRC) sitrep there are now 808 confirmed cases (973 suspected) of the Bundibugyo strain of Ebola detected. This is up (increased) from 544 suspected cases on June 8th. 192 deaths have been confirmed, up from 91 over the same time period.While the outbreak remains centered in the Mongbwalu, Bunia, and Rwampara health zones of Ituri district in northeast DRC, cases have been detected as far north as Aru, on the northwest Ugandan border, and as far south as Goma and Miti-Murhesa on the western border of Rwanda. The potential exposure landscape is vast. Although the outbreak was only officially declared on May 15th, about a month ago, this is already the third largest recorded outbreak of Ebola, trailing only the 2018–2020 Kivu outbreak in DRC and the 2013–2016 West Africa outbreak, each of which took years to contain. Modeled predictions from the CDC as of June 11th, indicate that real potential exists for this outbreak to become as serious or worse than the 2013-16 outbreak.
There is a certain degree of cold realism to be found in the hard numbers of case counts and treatment centers, reflecting a basic belief in the ability of health systems to understand events and exert control over a chaotic health crisis, but the early stages of this outbreak have been marked by enormous levels of uncertainty. As the WHO and the DRC government note, the virus was likely circulating for several weeks prior to the official declaration, which has made early stage containment efforts difficult. New cases are being detected routinely with no known chain of transmission, indicating that the detected cases may only be a small percentage of total contact pathways across an uncertain geography. The case fatality rate is currently unknown given the significant number of investigations underway into deaths which occurred prior to the outbreak declaration.
Making matters worse, this outbreak is being shaped in real time by several distinctive features which compound one another and increase the complexity of epidemic control efforts (WHO Ebola Outbreak 2026). For one, the Bundibugyo strain is relatively rare, as compared to the more common Zaire strain. Indeed, this is only the third documented Bundibugyo outbreak on record, and by far the largest, which is part of why the response toolbox is so thin. As of now, despite rapid ongoing research, there is no approved vaccine or therapeutic for Bundibugyo, though WHO advisory groups have prioritized several candidate vaccines and treatments for evaluation in emergency clinical trials. For now, clinical supportive measures and public health mitigation efforts are being implemented. PPE and sanitation supplies to prevent the infection of health workers are in high demand. The lack of vaccines and therapies makes non-pharmaceutical interventions, such as safe and dignified burials to mitigate the virus at its point of maximum contagion, all the more important.
The outbreak is also occurring in an area of eastern DRC which has been a conflict zone for some time. High security concerns and low levels of community trust have already placed medical and humanitarian response professionals in significant danger, above and beyond the risk of disease transmission, while elevating the seriousness of access constraints in outbreak affected and at-risk areas. Communities who are facing both ongoing conflict and the direct consequences of the outbreak continue to have mistrust of humanitarian organizations and government responses. This is because public health prevention intervention often conflicts with cultural practices, and because the area already has a range of under-resourced public health challenges. This often leads to misalignment of community needs and perceptions with epidemic control measures. At worst this results in violence, as evidenced by a set of recent security incidents at Ebola Treatment Units.
An Incomplete But Experienced Local Response
While the situation appears bleak in many respects, there are key advantages available to responders this time which either did not exist in previous outbreaks, or which previously had been underdeveloped. On the side of the public health response system in DRC and other parts of Eastern and Central Africa:
- Laboratory systems are working steadily through the backlog of testing samples for suspected cases and suspected deaths to get a more accurate view of the scope of the epidemic. Some of the initial high numbers of suspected cases ended up testing negative.
- Contact tracing, while far off the numbers needed to stem the outbreak, is improving. The most recent public estimate of contacts traced from the DRC MOH is 57%, which has improved from roughly 45% according to WHO only a couple of weeks ago.
- DRC and Uganda’s Ministries of Health have seen this before; both countries have trained a significant number of Ebola responders, and they are well prepared to know what to do based on multiple epidemic responses. Experienced Ebola responders from Guinea (Francophone), Sierra Leone and Liberia (Anglophone) are deploying to assist.
- While the initial delay in epidemic detection was highly unfortunate, it was nevertheless declared a Public Health Emergency of International Concern (PHEIC) just two days later, on May 17th — far faster than in the 2013–2016 West Africa epidemic, where the PHEIC came only in August 2014, many months after the first cases.
- Despite uncertainty, the case fatality rate among confirmed cases so far appears to be lower than previous epidemics of Bundibugyo; this may change as sample backlogs are tested.
Central and Eastern Africa have invested significantly in Ebola preparedness and response over the past decade. The resources available to local health agencies and governments are not close to sufficient, but these systems are working even if incompletely.
Digital Humanitarians And Data Gaps
Meanwhile, global digital humanitarians and remote data providers have begun to heed the call to “fight Ebola with information”. Almost immediately following the epidemic declaration, Humanitarian OpenStreetMap Team (HOT) coordinated with Médecins Sans Frontières to launch a set of tasks for the global digital mapping community to use high resolution satellite imagery to update building footprints, roads, critical infrastructure, and other features for the creation of maps to aid in population estimations, community surveys, contact tracing, and other epidemic control efforts. Their efforts have been buttressed by releases of satellite imagery from Vantor. Satellogic and Planet have also made satellite imagery available.
Other key organizations have stepped forward as well. Flowminder has been regularly publishing analysis of human mobility flows to and from the epidemic affected areas based on digital device data from the mobile network operator Vodacom. These flow maps allow for rapid prioritization of epidemic control efforts based on anticipation of probable case transmission areas. WorldPop and GRID3 have published high resolution baseline population data as well as accurate health facility locations to aid with planning for health services and calculations of baselines for population exposures, among other essential analyses. The Armed Conflict Location and Event Data (ACLED) project is publishing regularly updated geospatially specific conflict data to assist in understanding changing security risks and other threats to affected communities and to the response effort. UN OCHA’s Humanitarian Data Exchange (HDX) platform is now hosting more than 40 datasets specifically relevant to the current response in DRC, although a reasonably high number of these are topically filtered extracts from OpenStreetMap.
If we look above the proverbial “water line” of the information iceberg at what is publicly visible, easily traceable, and known to be in use by response actors, we can see significant gains in key areas. These include small area demographics, building footprint and infrastructure mapping, remote sensing, event alerting, and case reporting.
Right at the waterline, where novel datasets and models are emerging now into routine visibility and usage, we find human mobility flows based on mobile device data. Flowminder’s data from Vodacom has been integrated into several risk models. At this level we also see a range of disease forecast models and dashboards, at different levels of spatial and temporal resolution, some of which may be based on very similar data and distributed across opaque and discontinuous channels.
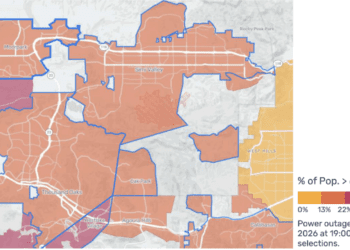
What is most concerning though is what still lies below the waterline, where needs may be unmet and substantial gaps in data, information, and analysis likely exist. For instance, as of now there does not appear to be a common list of ebola treatment units available publicly. Data on safe burials is largely absent. Misinformation, as is now normally the case online, runs rampant without an obvious rumor cataloguing effort, or community information management. Logistics and supply chain needs are referenced constantly by response agencies, particularly for PPE and sanitation, but supply chain flows are largely undocumented publicly, and in any event not obviously connected to the epidemiological forecasts and risk assessments despite clear calls from WHO for strategic prepositioning of essential supplies. Health facility locations are widely circulated, but facility-level capacity in terms of staffing, equipment, and supplies, is ambiguous at best. Epidemiological forecasts and risk analyses are not obviously connected to any particular workflows on logistics and supply chain.
Systems for surfacing and coordinating information management across the affected health zones in DRC, measured by staffing and organizational activity, is a thin patchwork right now. Local knowledge by response agencies and community leaders contributes in significant ways to epidemic control, but local actors also require resources to be effective. According to the Health Cluster’s “gap analysis” published on June 11th, while all of the affected zones have surveillance teams present, roughly half have no coordination structure in place, nor laboratory testing and logistics coordination. This analysis echoes calls made by MSF and others for an urgent scale-up of testing and supply chain activities in particular. Across the “pillars” of activity laid out by the UN, no health zone is considered to be adequately staffed, although the designations used by the Health Cluster tracking system could stand to be made more precise.
Linking Local Knowledge and Global Support
It is difficult but entirely possible, with a combination of local leadership and global support, to overcome the types of risks and complexities currently evident in DRC, and to extinguish the spread of this deadly disease (WHO West Africa Ebola). The hard work of field epidemiology combined with digital tools and data has been proven elsewhere to make a real difference. In order to do so efficiently and effectively though we have to strive to the best of our collective abilities to act and coordinate on the basis of high-quality, integrated data and information.
The reality is that these goals are intentionally ideal, because the response requires it. But in practice we have to be able to understand case detections relative to contacts and other factors like population mobility and density, so that health officials can place teams and resources appropriately. We have to connect that evolving transmission network to the needed health infrastructure, staff, and resources to provide efficient and effective health care, and to implement non-pharmaceutical epidemic interventions. We have to understand why, where, and how often safe and dignified burials are being refused, so that we can become better at convincing family members to protect themselves during end-of-life customs. The landscape of care and treatment has to be linked to the landscape of logistics and supply chains which make possible the movement of essential health commodities like personal protective equipment (PPE) at appropriate scales in a timely fashion to frontline areas. All of these models and workflows have to be contextualized within data on regional transportation and human mobility flows, infrastructure, communications networks, and population dynamics, as well as security risks and events and physical hazards like flooding which may disrupt response activities and redirect population movements at critical times and places. All of these calls place people and communities at the center of the response – from local actors to global donors. This is what the data and information landscape can be in its ideal form: a means to help bring communities affected by this health and humanitarian crisis to live healthier and more fruitful lives alongside humanitarian responders, government health workers and more – enhancing safety and support along the way.
Why are these various actions not happening to the degree that would be needed to stop the current epidemic? The reasons are many. Community trust is difficult to win and to retain even under the best of circumstances. Conflict and long-term complex humanitarian emergency contexts make that trust even more challenging, while also making the most basic things like safe movement of people and goods a daily struggle. At the same time, as has been well-documented elsewhere, the humanitarian funding landscape remains in disarray following the destruction of USAID and the redirection of resources by a number of governments in the EU from aid towards defence and other priorities. There is simply no current catalog available of the USAID systems and datasets which played important roles in previous outbreaks, but were taken offline by the Department of Government Efficiency (DOGE) in early 2025. Moreover, no current map or list exists of the data outputs from those systems which would have served as inputs into other systems. We therefore do not know the full extent of what was lost.
A Call To Action for Ebola Data
The time is now to map the datasets and systems in order to bring the digital information landscape into clearer view, to make it easier to access, and to render more transparent the shape of the absences that may now be affecting conditions on the ground.
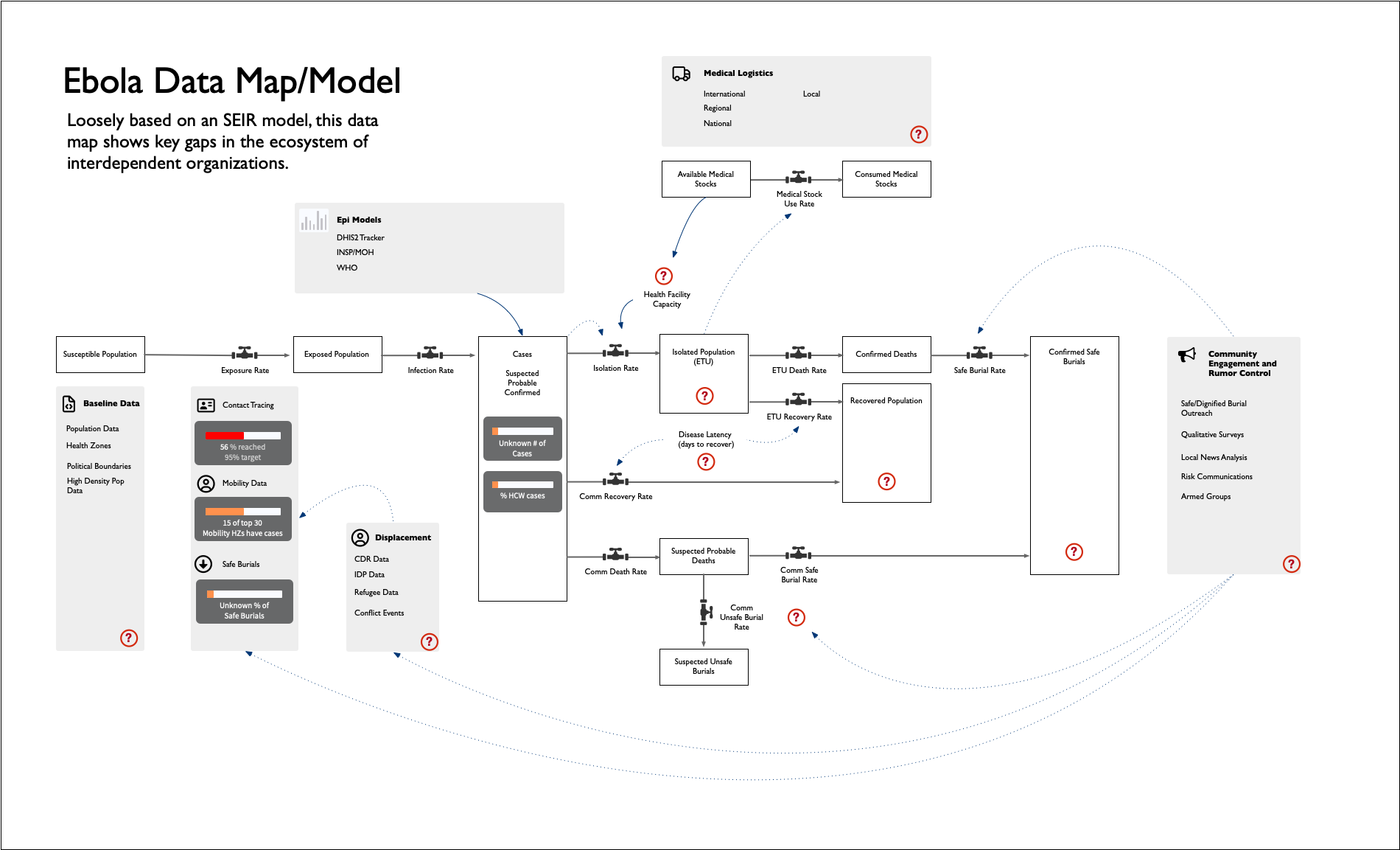
We have begun to compile a database of information sources and datasets which are now used, and have been used in the past by humanitarians, logisticians, modelers, and others, to stop Ebola outbreaks, particularly in DRC. In addition to the datasets themselves, we have begun to map these datasets to the principal known workflows and models for Ebola, to begin to understand what may be in need of replacement or repair. We are comparing this database of datasets to work that has been undertaken over the past year or so to understand where humanitarian data has been placed most at risk by the recent shocks to the international systems.
This compilation of resources is in no way intended at this point to be a complete archive. We recognize the limits of our own vision and understanding. Some systems and datasets, including for instance operational data specific to individual agencies, may not be publicly available. Some, including archives of satellite and drone imagery, may be available only by invitation to limited numbers of individuals and groups. Field surveys and contact tracing networks may only just now be in formation and beginning to circulate. Nevertheless, we as a digital humanitarian community need to take this moment to provide shape and structure to this landscape of data and information as well as we are able.
This letter is an open invitation to humanitarian response agencies and scientists to share what they know. The need for a more complete picture of activities, capacities, needs, and disease surveillance is urgent. Where are we missing important datasets? Which models are being used that we haven’t recorded here? Who has updated workflows in the response which are not broadly known, and which need support? And how is the information in these datasets and models being integrated into operational decision-making — aiding the field coordinators and logistics managers who hold far more context at their fingertips? Where they have that context, how can the global data and information community provide them with targeted, timely answers in support of the decisions they make?
Past experience shows that ebola outbreaks are unforgiving, but they can be stopped. The cost of inaction is high, but we can still mobilize to prevent the worst case scenarios. We need to act now though, or we are likely to regret it.
View the Ebola Data Map/Model PDF: https://www.crisisready.io/wp-content/uploads/2026/06/ebola_pillars.pdf
Figures
References
Official situation reports and statements
- INSP (Government of DRC), Situation Report N°30 — Maladie à Virus Bundibugyo, 13 June 2026. https://insp.cd/sitrep-n30-mvb_13-06-2026/
- WHO, Joint statement by the Government of the DRC and WHO concerning the outbreak of Ebola disease caused by the Bundibugyo virus, 31 May 2026. https://www.who.int/news/item/31-05-2026-joint-statement-by-the-government-of-the-democratic-republic-of-the-congo-and-who-concerning-the-outbreak-of-ebola-disease-caused-by-the-bundibugyo-virus
- Centers for Disease Control and Prevention, “Modeled Scenario Projections for the Ebola Disease Outbreak Caused by Bundibugyo Virus, 2026”, Mortality and Morbidity Weekly Report (MMWR) 11 June, 2026. https://www.cdc.gov/mmwr/volumes/75/wr/mm7522e1.htm
- WHO, Ebola outbreak — DRC 2026 (situation page). https://www.who.int/emergencies/situations/ebola-outbreak—drc-2026
- WHO, Ebola outbreak 2014–2016 — West Africa. https://www.who.int/emergencies/situations/ebola-outbreak-2014-2016-West-Africa
- Medicins Sans Frontieres, “DRC: One month on, MSF warns dangerous gaps persist in Ebola disease response”. https://www.msf.org/drc-msf-warns-dangerous-gaps-persist-ebola-disease-response
- International Federation of Red Cross and Red Crescent Societies (IFRC), “The International Red Cross and Red Crescent Movement expresses concern over attack on Red Cross volunteers in Bunia, Democratic Republic of the Congo (DRC)”, 5 June, 2026. https://www.ifrc.org/press-release/international-red-cross-and-red-crescent-movement-expresses-concern-over-attack-red
- Mercy Corps, “Ebola in Mongbwalu and Rwampara Epidemiological Trends, Community Perceptions and Challenges to Community Engagement in the Response”, 16 June, 2026. https://reliefweb.int/report/democratic-republic-congo/ebola-mongbwalu-and-rwampara-epidemiological-trends-community-perceptions-and-challenges-community-engagement-response
News and analysis
- Deutsche Welle, “Ebola: WHO’s Tedros visits Uganda, bordering DRC epicenter,” 8 June 2026. https://www.dw.com/en/ebola-outbreak-whos-tedros-visits-uganda-bordering-the-drc-ituri-province-epicenter/a-77462569
- CIDRAP, “Ebola outbreak reaches 550 cases, at least 90 deaths.” https://www.cidrap.umn.edu/ebola/ebola-outbreak-reaches-550-cases-least-90-deaths
- NPR, “Ebola outbreak, trust, death and burial in the DRC,” 29 May 2026. https://www.npr.org/2026/05/29/g-s1-124359/ebola-outbreak-trust-death-burial-democratic-republic-congo
- NPR, “In his book, self-described USAID ‘whistleblower’ talks about the agency and Ebola,” 8 June 2026. https://www.npr.org/2026/06/08/g-s1-125269/ebola-usaid-outbreak-trump-musk-woodchipper-nicholas-enrich
- ABC News, “DRC reports record number of Ebola cases in a single day.” https://abcnews.com/Health/drc-reports-record-number-ebola-cases-single-day/story?id=133883214
Data, mapping, and analysis platforms
- Humanitarian OpenStreetMap Team, DRC Ebola 2026 mapping tasks. https://wiki.openstreetmap.org/wiki/Humanitarian_OSM_Team/Open_Mapping_Hub_Eastern_and_Southern_Africa/DRC_Ebola_2026
- Flowminder, Population movements from Bunia, Mongbwalu and Rwampara (Vodacom Congo mobile data). https://www.flowminder.org/resources/publications-reports/drc-reports-publications/population-movements-from-bunia-mongbwalu-and-rwampara-based-on-privacy-secure-analysis-of-mobile-operator-data-from-vodacom-congo
- Cluster EHA, “Ebola RDC 2026 – Carte de response WASH (15 June 2026). https://ibagur.github.io/IM-portfolio/outputs/drc/drc_ebola_dashboard.html#page-1
- WorldPop, WOPR — DRC population. https://wopr.worldpop.org/?COD/Population
- GRID3, COD Health Facilities v8.0. https://data.grid3.org/datasets/GRID3::grid3-cod-health-facilities-v8-0/about
- ACLED, DRC conflict data. https://acleddata.com/country/democratic-republic-congo
- UN OCHA HDX, Ebola — Bundibugyo virus disease (crisis page). https://data.humdata.org/event/crisis-ebola-bundibugyo-virus-disease
- Health Cluster (ReliefWeb), RDC — Analyse des gaps dans les zones de santé touchées et menacées par la MVD, au 01 juin 2026, published 11 June 2026. https://reliefweb.int/report/democratic-republic-congo/rdc-health-cluster-analyse-des-gaps-dans-les-zones-de-sante-zs-touchees-et-menacees-par-la-mvd-au-01-juin-2026
- ReliefWeb, Fighting Ebola with Information: Learning from the use of data, information, and digital technologies in the West Africa Ebola response, 20 January 2017. https://reliefweb.int/report/liberia/fighting-ebola-information-learning-use-data-information-and-digital-technologies
Project resources
- [Internal] Ebola dataset database (Google Sheet). https://docs.google.com/spreadsheets/d/1kVtI4AhgqW2XAMc2Vgzs8jhs1v0CQP0c/edit?usp=sharing